Hemorrhoids Online Registration
An anal fistula is an infected tunnel under the skin that connects the anal canal and the surface of the surrounding skin. The majority of fistulas occur as a result of an anorectal infection that led to pus-filled cysts to form near the anal canal and spread to the skin.
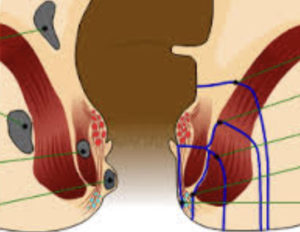 Because anal fistulas are classified by their location in relation to the anal sphincter muscles (intersphincteric transphincteric, suprasphincteric, and extrasphincteric fistula), diagnosis first requires your doctor to locate the external opening of the fistula. Using an anoscope and a probe to identify the fistula path, your doctor will diagnosis you with one of the following four fistula types:
Because anal fistulas are classified by their location in relation to the anal sphincter muscles (intersphincteric transphincteric, suprasphincteric, and extrasphincteric fistula), diagnosis first requires your doctor to locate the external opening of the fistula. Using an anoscope and a probe to identify the fistula path, your doctor will diagnosis you with one of the following four fistula types:
Deemed the Parks classification, these four distinctions are based on the location and path of the fistula. Moreover, anal fistulas are described as either simple or complex. Simple fistulas are low transsphincteric and intersphincteric fistulas, while complex fistulas describe any other type of fistula, which can take many shapes, sizes, depths and directions. Fistulas that are NOT categorized as one of the above four types are known as superficial fistulas, which are not linked to the anal canal or the sphincter.
Symptoms
Uninfected anal fistulas usually cause anal itching and drainage from the opening of fistula. Infected anal fistulas cause fever and returning abscesses with a constant, throbbing pain; symptoms worsen with movement, passage of stool, and coughing/sneezing. The extreme discomfort caused by infected fistulas tends to make digital rectal examinations difficult without use of an anesthetic. In many cases, more advanced diagnostic methods are necessary.
Treatment
Treatment for anal fistulas varies depending on the severity and location of the fistula. Antibiotics, antipyretics and pain medication are prescribed if there is drainage (indicating an abscess). When treating fistulas, the goal is to alleviate the problem without affecting the sphincter muscles.
For simple fistulas, a fistulotomy or fistulectomy is typically performed. These surgeries either clear out the fistula tract or completely remove the tract to allow the area to fully heal. During a fistulotomy, your doctor probes to find the fistula’s internal opening. The tract is then cut open and scraped clean. The wound is either left open or is stitched in a way that the fistula is laid open. During a fistulectomy, your doctor may only open up the segment where the tracts join and remove the remainder of the tracts. This procedure can be completed in more than one stage or repeated if the entire tract can’t be found.
More complex fistulas that twist and branch out are tougher to treat using a traditional fistulotomy or fistulectomy. Patients are usually referred to a colorectal surgeon for further evaluation and treatment. Treatment options for complex fistulas include a fistulectomy with advancement rectal flap, a seton placement, and fibrin glue.

